Serving All North Carolina
(704) 954-8697
What Are the Most Common Workplace Injuries Among Healthcare Workers?
Connect With Us
19Jun
Healthcare workers are injured on the job at rates that rival or exceed construction and manufacturing — a fact that surprises many people who associate occupational hazard with physically dangerous industries rather than hospitals and clinics. According to the U.S. Bureau of Labor Statistics, healthcare support occupations and nursing assistants in particular experience some of the highest rates of musculoskeletal injury of any occupational category tracked, with patient handling identified as the most commonly cited single cause of occupational injury in the healthcare sector.
Understanding which injuries occur most frequently, and why, helps healthcare workers recognize risk patterns and understand what workers’ compensation covers when an injury occurs.

Patient Handling: The Leading Cause of Healthcare Worker Injury
Lifting, repositioning, and transferring patients is physically demanding work involving unpredictable loads. Unlike lifting a box of known weight from a fixed position, moving a patient requires accounting for the patient’s own movement, their ability or inability to assist, equipment in the way, and confined spaces that limit proper body mechanics.
The physical tasks that most consistently increase injury risk involve manual patient transfers: moving a patient from bed to wheelchair, repositioning a patient in bed to prevent pressure injuries, and assisting patients who are partially weight-bearing but unstable. These tasks generate forces on the lower back, shoulders, and knees that exceed what manual lifting guidelines consider safe, particularly when performed repeatedly across a shift without adequate mechanical assistance.
Common patient-handling injuries include:
- Lower back strains and disc injuries from lifting and repositioning without adequate support
- Shoulder injuries, including rotator cuff tears, from repeated overhead reaching and transfers
- Neck strain from sustained awkward postures during patient care
- Knee injuries from twisting movements while supporting patient weight
- Cumulative trauma disorders that develop over months or years of repetitive patient handling
OSHA has issued specific guidance on safe patient handling, recommending that healthcare facilities implement mechanical lift programs rather than relying on manual lifting techniques, which research has shown do not adequately protect workers regardless of how carefully they are performed.
Slips, Trips, and Falls in Healthcare Settings

Hospital and clinic floors present hazards that are less obvious than they might seem. Spilled fluids, wet floors from cleaning, cluttered hallways, and the fast pace of emergency response all contribute to slip and fall risk. Healthcare work-related injuries from falls range from minor sprains to serious fractures, particularly when a worker falls while carrying equipment or assisting a patient.
Night shift workers face elevated fall risk due to lower lighting and fatigue. Workers moving quickly between patient rooms, managing multiple competing demands, face more unpredictable walking surfaces and less predictable pacing than workers in most other settings.
Needlestick and Sharps Injuries
Needlestick injuries remain a persistent risk despite decades of safety engineering improvements. A needlestick injury exposes a worker to bloodborne pathogens, creating both an immediate physical injury and a potential infectious disease concern that requires follow-up testing and, in some cases, prophylactic treatment.
The Needlestick Safety and Prevention Act requires healthcare employers to use engineered sharps injury protection devices and maintain a sharps injury log. Despite these requirements, the Centers for Disease Control and Prevention estimates that healthcare workers experience approximately 385,000 needlestick and sharps injuries annually in the United States.
After a needlestick injury, workers should wash the area immediately and thoroughly, report the incident to a supervisor and occupational health right away, identify the source patient for testing when possible, and undergo baseline and follow-up testing at defined intervals. Post-exposure prophylaxis may be appropriate depending on the source patient’s status and the nature of the exposure.
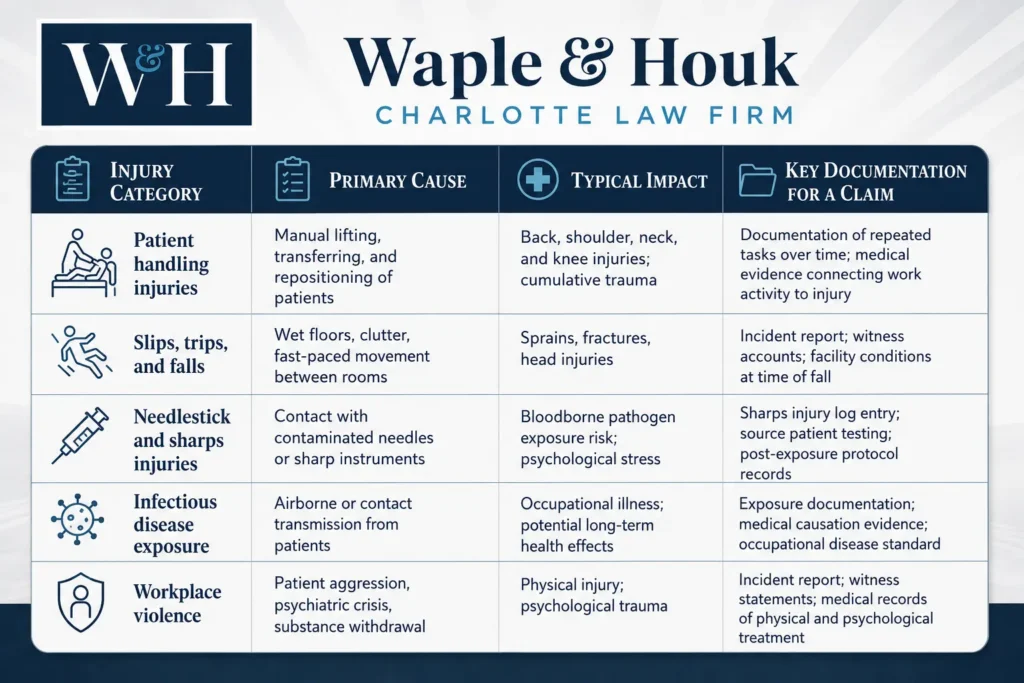
Infectious Disease Exposure as an Occupational Hazard
Beyond sharps injuries, healthcare workers face ongoing exposure to airborne and contact-transmitted infectious diseases. This risk became broadly visible during the COVID-19 pandemic, but it predates and continues beyond that event. Tuberculosis, influenza, hepatitis, and other communicable diseases present ongoing occupational exposure risk for workers who work directly with patients.
When an infectious disease exposure results in illness, North Carolina workers’ compensation law treats this as an occupational disease claim rather than a traumatic injury claim. The legal standard requires showing that the disease is characteristic of and peculiar to the worker’s occupation and that the occupation was a significant contributing factor in causing it. For healthcare workers whose direct patient contact created clear exposure pathways, this standard is often met — but the claim still requires medical and occupational documentation connecting the exposure to the resulting illness. Workers facing disputed occupational disease claims often benefit from legal support in building that documentation.
Workplace Violence in Healthcare Settings
One of the most underrecognized hazards in healthcare worker injury data is workplace violence. Healthcare and social assistance workers experience workplace violence at rates significantly higher than nearly any other industry, driven by patient confusion or agitation related to medical conditions, mental health crises, substance withdrawal, and the emotionally charged environment of emergency departments and psychiatric units.

Workplace violence injuries in healthcare are frequently underreported, in part because healthcare workers sometimes view patient aggression as part of the job rather than a compensable workplace injury. That assumption has real consequences: claims go unfiled, injuries go undocumented, and workers absorb costs they were legally entitled to have covered. Reporting a work injury, including one caused by patient violence, is the first step toward protecting those rights. An assault by a patient — even one whose condition makes them not legally culpable for the act — is generally a compensable workplace injury under North Carolina law when it occurs in the course of employment.
Common workplace violence scenarios in healthcare include physical assault by confused or agitated patients, particularly in emergency departments and dementia care units; violence during psychiatric crisis intervention or substance withdrawal management; assault from family members or visitors under emotional distress; and verbal threats that escalate to physical contact during high-stress care situations.
Why Healthcare Workers Face Elevated Injury Risk

Several factors converge to make healthcare workers’ injury rates higher than many physically demanding industries with more obvious hazard profiles. Healthcare work combines unpredictable physical loads, unpredictable patient behavior, biological hazard exposure, long shifts that produce fatigue, and a culture that in some facilities still implicitly discourages reporting minor injuries in favor of pushing through.
Staffing levels play a significant role. When patient-to-staff ratios stretch thin, individual workers handle more patient transfers, more emergency responses, and more physically demanding tasks per shift — increasing cumulative exposure to the activities that cause injury. Charlotte’s growing healthcare sector, anchored by major hospital systems including Atrium Health, Novant Health, and Carolinas HealthCare, reflects the same national patterns in injury risk that exist throughout the industry.
Workers’ Compensation Benefits for Healthcare Worker Injuries
North Carolina workers’ compensation covers healthcare workers injured in the course of their employment the same as workers in any other field, though the specific patterns of injury common in healthcare — particularly cumulative trauma and occupational disease claims — sometimes face more scrutiny than acute traumatic injuries with a clear single cause.
A back injury that developed gradually over years of patient lifting is a legitimate workers’ compensation claim, but it requires documentation establishing the connection between cumulative work activity and the resulting condition. This is different from, and often more challenging than, documenting an injury that resulted from a single identifiable incident.
Workers’ compensation benefits available to injured healthcare workers include coverage for medical treatment, wage replacement during periods of disability, and compensation for permanent impairment when applicable. Workers who cannot return to direct patient care due to injury restrictions may also have long-term wage loss claims available depending on the nature of the restriction and whether suitable alternative work exists. Psychological effects from workplace violence or traumatic exposures can also be part of a workers’ compensation claim when properly documented.
If You Have Been Injured Working in Healthcare

The injuries that healthcare workers sustain are not inevitable consequences of choosing this career. They are well-documented occupational hazards with established legal protections. Workers who treat a patient assault, a back injury from a lift, or an infection exposure as simply part of the job sometimes leave legitimate claims on the table — benefits that were designed specifically to protect them.
Understanding the workers’ compensation claims process is a practical starting point, particularly for cumulative trauma and occupational disease claims where documentation requirements are more involved. At Waple & Houk, our team has experience with the specific injury patterns that affect healthcare workers and can help you build the record a successful claim requires. Contact us for a free consultation.
Workers’ Compensation
And Family Lawyers
Providing
Strength In A
Time of Crisis
Call US now:
Our Success
Case Results
$80,000
Elbow Injury
$350,000
Arm Injury
Related Posts


reviews
What Real Clients Have To Say
Melissa S.
Lou and his team did an outstanding job on my case. They kept me updated constantly. There were times when I was so overwhelmed-the encouragement I received from the firm is the BEST I’ve received from any law firm in the past. I HIGHLY recommend Lou and his team.
Tim J.
Great attorney helped the most at a important time.
Aimee B.
Lou and his team worked quickly to ensure that my husband received the care and physical therapy he needed after a pretty serious work injury. They handled every phone call and question with the insurance adjuster, we didn’t have to fight with anyone to get anything that was expected or promised. They communicated with us every step of the way, and they were especially responsive and helpful when my husband’s case required more than anyone had anticipated. Every person we have spoken with in Lou’s office were patient and respectful, we never felt like we...
Lucas J.
Very good people to work with! I highly recommend this law firm.
Dustin M.
I have never had a more pleasant experience with an attorney and their paralegals in my life!!! Hands down the best law firm in North Carolina, probably the whole country! Would definitely recommend them to anyone needing counsel. They are all so easy to get along with and friendly.... My employer lied, as many do in this situation but Lou and his team were quick to step in and get me the compensation I deserved! Thank you, from my whole family. Waple and Houk are #1
Darrin R.
Mr. Lou is by far the most compassionate attorney I’ve encountered and once again he helped me with a worker’s compensation claim and his paralegal was also great. Mr.Lou is very professional and he allows you room for your concerns and opinions, he’s just a great human being that doesn’t need to advertise his partnership law firm on tv just ask any of his past clients and they would totally agree with me, God forbid that I’m in a serious car accident but if I am he’s just a phone call away so if you...
Travis B.
Mr. Waple did a fantastic job on my case, even if I wasn't a lot of help he still came through and for that I thank you Mr. Waple.
Tara D.
I was at a point of despair & thought that my then employer would do the right thing. Lou’s honesty, and integrity; along with his guidance gave me the dose of reality that I needed to see the true colors of legality in corporate America. Without his savvy I would have been blindsided! Cherie, always responded to all of my responses, and nervous reactions and made sure Lou was aware of what was happening! Great firm, I would highly recommend to anyone who wants respect, honesty and guidance as a client!
Aunyette S.
Mr.Waple has handled both of my cases very well. I definitely recommend this team of professional lawyers and secretaries. Thank you!
Tashaun H.
My experience working with Lou was an absolute joy. From our very first conversation, he assured me that he would work relentlessly to help me secure adequate compensation for my case and he did just that. His paralegal, Cheri, was helpful with timely responses to any and all questions I had and she helped reduce the stress of a very tedious process. I highly recommend this firm for any future litigation and would love to work with them again if the opportunity arises.

Request a Consultation
We Are Here For You
Copyright 2026 All Rights Reserved | Accessibility Notice | Privacy Policy
Attorney Advertising. This information is designed for general information only. The information presented should not be construed to be formal legal advice nor the formation of a lawyer/client relationship. Past results and testimonials are not a guarantee, warranty, or prediction of the outcome of your case, and should not be construed as such. Past results cannot guarantee future performance. Any result in a single case is not meant to create an expectation of similar results in future matters because each case involves many different factors, therefore, results will differ on a case-by-case basis. By providing contact information, users acknowledge and give explicit consent to be contacted via the methods of communication provided, including SMS. Message and data rates may apply. Message frequency may vary. Reply STOP to opt out.
